The American Medical Association (AMA) loves to celebrate its legislative victories. “AMA defeats 100 pieces of legislation to expand midlevel practice authority“, they announce, as if they’ve permanently solved the problem of Nurse Practitioners (NPs) and Physician Assistants (PAs) seeking greater autonomy. But then, inevitably, more bills appear in different states. The same fight erupts again. The AMA mobilizes again, spends resources again, claims victory again. Only to watch the cycle repeat.
Perhaps that sounds familiar to anyone who’s worked in a hospital. It’s the clinical equivalent of a resident who sees a feverish patient, orders Tylenol, and sends them home, only to have the same patient return with persistent fever. More Tylenol. Patient returns again. Stronger medications. The resident keeps escalating symptomatic treatment while completely ignoring the underlying infection that’s actually making the patient sick. When the patient eventually develops septic shock, everyone asks how they missed something so obvious.
There’s a cardinal rule in medicine that explains both scenarios: when the same problem keeps recurring despite your interventions, you’re probably treating symptoms rather than disease. It’s drilled into medical students, reinforced during residency, and yet even experienced physicians sometimes fall into this trap. The question is whether organized medicine recognizes that it’s been making this exact mistake on a population level for decades.
The term for the symptom, in this case, is scope creep, the expansion of practice authority for midlevel providers, mostly Nurse Practitioners (NPs) and Physician Assistants (PAs). In recent years, several states passed legislation to grant midlevel providers greater autonomy, and many more are considering them. These proposals are deeply unpopular with physicians1, on multiple fronts. First, midlevel providers typically have significantly less training than physicians, which has led poorer patient outcomes. Second, increased competition from midlevels who can practice at similar levels for half the salary would inevitably depress physician wages. Third, there’s the natural human tendency to protect your territory, especially in a highly skilled and somewhat egotistical field like medicine. There is an entire subreddit, r/noctor, that hates on Nurse Practitioners presenting themselves as “doctors”.
Consider the AMAs efforts as a treatment. Why does “treating” these bills with lobbying only delay when it pops up? Why does this problem keep coming up again and again? Why do these bills even get considered? Is it possible that the AMAs treatments, like the resident’s Tylenol, are technically correct, but still completely missing the point?
The disease, many will be quick to point out, is greed. NPs and PAs are happy to take the higher wages that come with expanded responsibilities. Health Conglomerates are pushing for these bills to cut on cost, and effort to save on physician costs, to screw over the patients for profit. And the government, as always, is capitulating to the whims of Big Business. As an anti-establishment lefty, these conspiracies were easy enough to for me to accept. Since they validated my world view, they had to be true!
The problem is, that explanation is wrong. To my surprise, physicians2 were the disease.
Solutions of the Past are Problems of Today
Some background: Contrary to what many physicians think, residents are NOT profitable, not even remotely, which is why only about 2% of residencies are privately funded. 98% of medical residencies are funded in some form by the government.
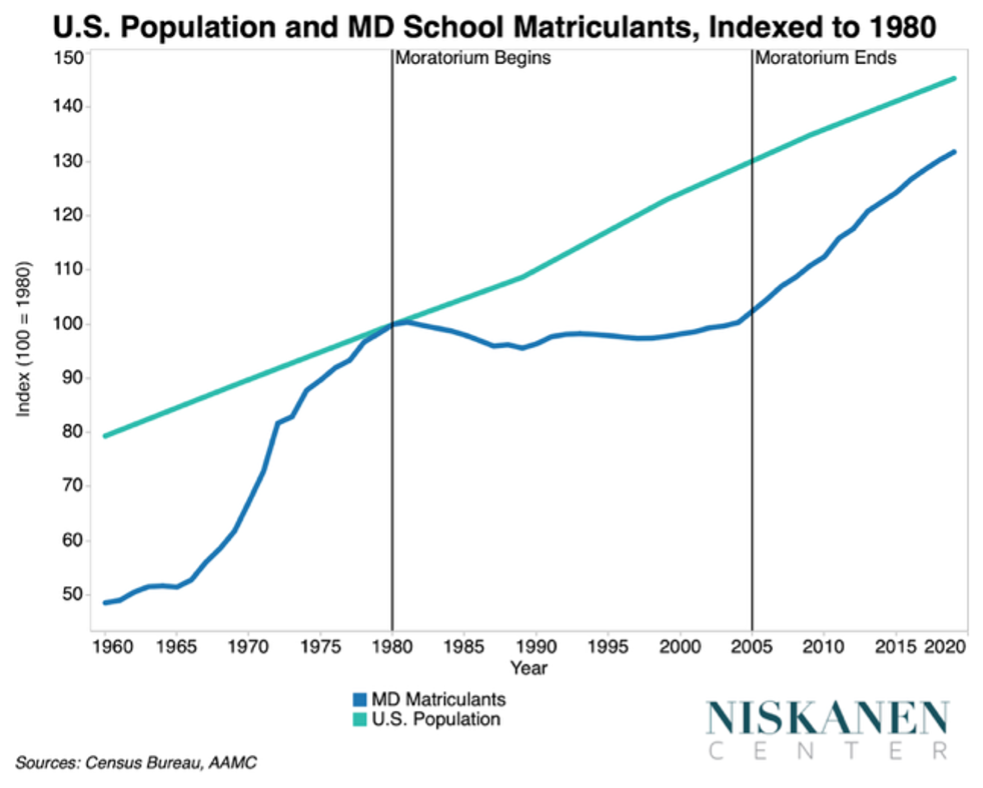
The story starts in 1981, with the Department of Health, Education, and Welfare commissioned the GMENAC report, which concluded that the United States was on the verge of a massive physician surplus. And my god, did the medical community lose its mind. In the next few years, every medical association and multiple government agencies were talking about a “surplus”. The AMA, the Association of American Medical Colleges (AAMC), and other medical associations came together to deal with this. They cooked up the Medical School Mortarium, where MD schools agreed to voluntarily reduce the number of applicants3. In the time this lasted, from 1980-2005, the population grew while the number of medical students slowly declined. Only three new MD schools opened at this time. (Nisaken Center).
In 1997, the AMA went to straight to the top. They lobbied Congress to cap this oncoming disaster of too many physicians. In Washington, balanced budgets were all the rage. It didn’t take much convincing for them to cap the number of federally funded residencies to 1997 levels in the Balanced Budget Act of 1997. (Nisaken Center). This, of course, completely fixed the budget and the US is no longer in debt (…right?).
The residency cap has remained virtually unchanged for nearly three decades.
Simultaneously, the AMA fights importation of foreign trained physician, or International Medical Graduates (IMGs). It is, after all, the American Medical Association. IMGs have much higher application fees, are required to do extra “Pathway” for certification, and are systematically ranked lower by residency programs. It doesn’t help that the country as a whole has become more anti-immigration as of late, so even after jumping through the hoops of the healthcare bureaucracy, they have to jump through the increasing hoops of the immigration bureaucracy. Yet nurses are treated as a permanent shortage occupation, so have a streamlined immigration process. This is why there are entire agencies, such as Nash Group, that recruit and place thousands of internationally trained nurses across the US.
Like everything, it’s just supply and demand. The supply side is full of limitations: limit number of medical students, limit the number of residencies, limit the number of IMGs. The demand side has skyrocketed: the US population has grown 70 million people in the last three decades and aged considerably. In any system where demand outpaces supply, there is a shortage. In this case, the worst shortage in the developed world – the US has fewer physicians per capita than any other developed nation. This has created an impossible situation for state governments, who control licensing requirements: they have literally no one to treat their populations.
Their calculus is simple: Physician > Midlevel >>>>>>>>>>>>> No Healthcare Provider.
States aren’t expanding midlevel scope out of preference or because of corrupt lobbying from big health systems. They’re doing it out of economic necessity. As long as healthcare demand of their populations continues increasing, they will take whatever means necessary to meet that demand. If physicians aren’t available, they’ll use nurse practitioners. If nurse practitioners need expanded scope to be effective, states will grant it.
This physician shortage is particularly severe in rural areas. Rural physicians have higher salaries4 , much lower cost of livings, and generous signing bonuses and loan repayment packages than their urban counterparts. Yet all that has failed to attract physicians to rural areas (NJEM). Since throwing more money at the physicians doesn’t work, midlevel scope expansion begins in these desperate rural states. Once a state grants nurse practitioners independent practice authority and the sky doesn’t fall, neighboring states take notice. This creates a cascading effect where each successful midlevel expansion makes future expansions easier and more normalized.
Physicians who can’t serve society’s needs will find society no longer needs them to serve.
This is why the AMA has pivoted in recent years. For the last 5 or so years, it has been lobbying Congress to increase residency positions and has supported several pieces of legislation to address the shortage. But, Congress, bless their hearts, has been having trouble doing any sort of legislation lately, due to increasing polarization for the last two decades. That’s not to say they haven’t tried!
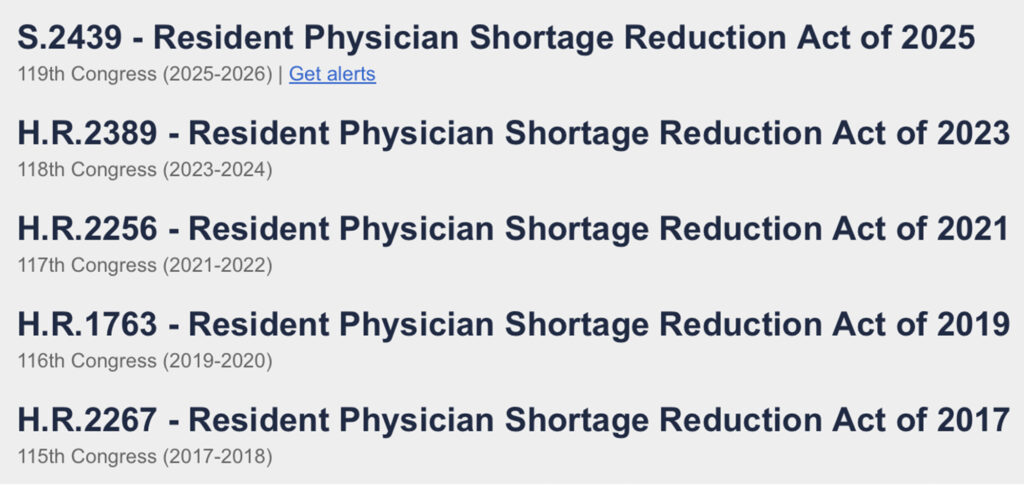
This is what you see when you search Congress.gov for “Resident Physician”. Check the cosponsors and you can see bills like this all had bipartisan support, came from both the Senate and House, yet never ended up passing. The AAMC keeps hyping them up, too! Check the AAMC news site and you’ll see articles such as “AAMC-Supported Bill to Address the Physician Shortage Introduced” posted in 2017, 2019, 2021, 2023, and 2025.
Physician’s Resistance to Reform
Beyond increasing the number of residency spots, physicians as a whole are resistant to broader structural changes that could meaningfully address the shortage.
The US medical education system is remarkably inefficient compared to international standards. A bachelor’s degree is required to apply to medical school, where acceptance rates hover around 2% for individual schools with only 40% of applicants gaining admission each cycle. This intense competition forces students to take an average of 2 gap years before applying, pushing the average age to start medical school to 24 (AAMC). Medical school itself takes 4 years, followed by mandatory residency training lasting 3-7 years, often with an additional 1-3 years of fellowship. Some students even take research years to strengthen their residency applications. The result? Physicians start as an attending is 30-32 years old US.
Compare this to UK, where medical school is a 5-6 year program directly after high school. After graduation, there is a two-year required internship, after which students can begin practicing as general practitioners independently, or choose to specialize further through residency training (EGMS). That means British physicians can start practicing independently at 25-26 years old, about 6 full years earlier than their American counterparts.
The standard argument is that the US system creates superior physicians. We select only the best and brightest for medical school. Students bring more life experience, advanced degrees, and greater maturity. Attending physicians have undergone many more years of rigorous training with extensive specialization options to hone individual expertise. I would agree with these points. They do probably produce better individual physicians. But from a public health perspective, 6 additional years of a good doctor will accomplish more than 6 fewer years of an excellent doctor.
Yet reforms to streamline American medical education would face extraordinary resistance. Removing the bachelor’s degree requirement would provoke such extreme outrage from physicians that it would be unthinkable. The AMA would spend every dollar to destroy such a proposal. Similarly, allowing medical school graduates to practice family medicine without an extended residency training would be considered an assault on medical standards, despite working successfully in countries like Germany. Let’s be honest about what these reforms represent: they are, in essence, lowering standards for physicians. And anything that “lowers standards” is extraordinarily unpopular among physicians, even when it could benefit society.
Here’s an even more drastic change: why not have the government dictate what locations and specialties newly trained physicians can practice based on what the greatest shortage is? The answer is the ultimate irony of physician autonomy: medical education being expensive and privately funded is actually physicians’ best defense against government control.
If medical education were subsidized or free, the government would have legitimate grounds to direct physician practice. The argument becomes simple: “The taxpayers funded your education, so you owe service to underserved areas”. That’s a common thing worldwide. Take Japan, which operates one of the world’s most successful physician workforce planning program. The government mandates the number of medical schools in an area and recruits students specifically from rural areas who are most likely to remain. Another program assigns physicians to specific regions for their foundation years in return for tuition (Human Resource for Health). The Japanese have greater access to doctors, and more leeway to deal rural physician shortages because they can influence service as a condition of subsidized education. Even within the United States, we see this principle in action, albeit on a much smaller scale. Military medical programs pay for students’ education in exchange for years of service at bases worldwide, and in return, it significantly constrains your choices based on service needs. Similarly, the National Health Service Corps provides loan forgiveness to medical students who commit to working in underserved areas for specified periods.
The current expensive, debt-financed system gives physicians their strongest argument for autonomy: “I paid for my own education with loans, so I can practice wherever and however I want”. A politician can’t easily argue a physician should be forced to work in rural Alabama as a family physician, when that physician personally borrowed a half-million dollars for their training. Any attempt for such a mandate would be met with extraordinary backlash from physicians in a way it just would not by physicians in other countries.
And that autonomy gives US doctors some great benefits, beyond just higher salaries. Want to spend more time in research rather than patient care? Go ahead! How about living in a remote beach house and do telehealth all day? Why not! Are you getting bored of your specialty? No problem! – just choose between 120+ fellowships/subspecialty programs.
This creates a catch-22 for addressing the physician shortage. Making medical education cheaper and more accessible would increase physician supply, but it would also give governments the leverage to direct where those physicians practice and what specialties they choose. Physicians have traded affordability for autonomy, and now find that autonomy under threat anyway due to market forces they set in motion.
The Blame Game
Now comes the fun part: deciding who to point the pitchforks at. The 1990s physicians who panicked about oversupply? Midlevels pushing for expanded scope? Healthcare corporations prioritizing profits? State governments caving to pressure? The federal government that created this cap? Or how about God, for giving us Covid that made this all worse?
Despite my criticisms throughout this piece, I don’t blame physicians for the current shortage. That argument was ragebait to keep you reading. The fear of oversupply wasn’t irrational; just look what happened to lawyers and pharmacists when their fields flooded with graduates5 . Is it wrong try to maintain high standards of patient care, professional autonomy, and high salaries? Are those not the things that attracted me to medicine, that keep me working through medical school? And the AMA has made a lot efforts to correct course in the last few years.
Can I blame NPs and PAs for seeking the higher salaries that come with autonomy as their own educational costs skyrocket? Hell, their lobbying organizations are far weaker than the AMA, so how much expansion really stems from their advocacy versus pressure from healthcare conglomerates? And much as I want to blame the corporations, I can’t fault them for lobbying when they literally cannot recruit enough physicians to meet demand. And I can’t blame states for yielding when their populations, especially rural communities, face deteriorating health outcomes.
Perhaps the federal government bears the most responsibility. But the 1997 Congress likely assumed they could easily adjust the residency cap later as needed. They couldn’t foresee today’s legislative gridlock. That would make the last decade’s Congress most at fault6 . But I know any drastic reforms like subsidized medical education would cost enormous sums no politician wants to fund and would trigger fierce medical profession backlash, making it politically toxic. Even raising the cap now is band-aid fix (although I expect it will happen in the next few years), which would take another decade to to feel the effects of.
We’re trapped in a system where every entity is acting rationally, yet their collective logic drives us further from the most rational solution. As long as the incentive structure remain the same, what can change?
- I use ‘physician’ rather than ‘doctor’ since many healthcare providers now hold doctoral degrees (PharmD, DNP, DPT), making ‘physician’ the precise term for medical doctors. ↩︎
- I use ‘physicians’ and ‘AMA’ interchangeably throughout this piece, which will irritate doctors who claim the AMA doesn’t represent them, given that only 17% hold memberships. But my conflation reflects reality: the AMA operates the essential infrastructure of American medicine.
Back in the day, any dipshit could call themselves a physician and prescribe cocaine for headaches. You know who lobbied for licensing requirements to change that? The AMA.
Who created the CPT billing codes all physicians use? The AMA.
Who co-accredits every medical school and heavily influences residency training standards through the LCME and ACGME? The AMA.
Disavowing the AMA as ‘not representing doctors’ while every single aspect of being a doctor exists because of AMA-influenced systems is intellectual dishonesty. The organization’s low membership rate simply proves it’s so institutionally powerful that individual doctors can enjoy its benefits without paying dues. If physicians were truly against the AMA, they would have formed their alternative organization. ↩︎ - This also explains why medical school admissions are getting more competitive. We are barely increasing the number of spots even as the population, especially the college educated population, has increased. The demand from premeds is high, so something will form to provide a supply – that’s why there has been a rise of DO schools. ↩︎
- The pay difference is not huge, maybe 5-10%, but there is a much lower cost of living, and a lot of other benefits. Anecdotally, you’ll find many doctors talking about getting paid twice amount in rural areas. ↩︎
- In both these fields, a ton of new schools opened up rapidly, decreasing student quality and oversupplying the market. The fields salaries tanked and the degree is worth less. ↩︎
- This blog post was (mostly) written before the One Big Beautiful Bill Act. It has heavy cuts to student loans which is going to be even worse for doctors. But since we’ve yet to see the effects of that, and since I didn’t want to completely change my ending, I have ignored the bill. There’s a great White Coat Investor post about the bills effects on physicians if you want to learn more. ↩︎
King you cooked, i like how comprehensive this is. You try to accommodate and consider a lot of view points. Also I concur, all parties are trying to make the best of a broken system yet choosing not deal with the problem at large. This struggle as well as many struggles society currently has to deal with agglomerate to the unfortunate reality that society at large moves for the bottom line.
I might just be a pessimist right now but I think that greed and self preservation tend to be stronger motivators than altruism and that is clearly highlighted here. It has more to do with intellectuals who realize the issue at hand and are worried about their own immunity than that of the world at large. It takes an upheaval of ideological change and action to fix intentional systematic issues like this; change that is often slow or never to happen unfortunately.
I will say that I mess with graph, I can see the fairly large amount of time u put into this gang and the generations lock in that this took. Peak gaf max.
I liked this style of writing for you as well. It was rather informal but that made it feel like a chat more than it did an expose which i’m sure is the goal.